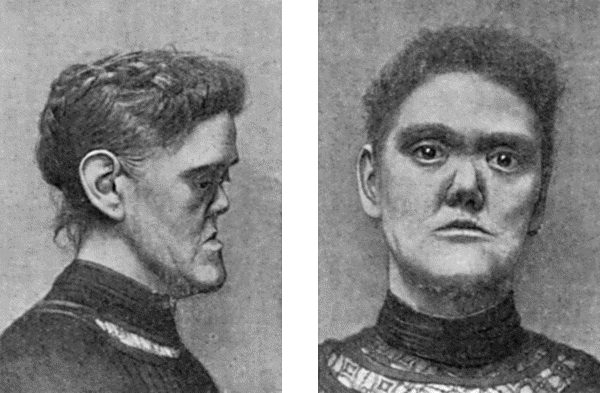
Fig. 43.—Facies of Inherited Syphilis.
(From Dr. Byrom Bramwell's Atlas of Clinical Medicine.)
One of the most striking features of syphilis is that it may be transmitted from infected parents to their offspring, the children exhibiting the manifestations that characterise the acquired form of the disease.
The more recent the syphilis in the parent, the greater is the risk of the disease being communicated to the offspring; so that if either parent suffers from secondary syphilis the infection is almost inevitably transmitted.
While it is certain that either parent may be responsible for transmitting the disease to the next generation, the method of transmission is not known. In the case of a syphilitic mother it is most probable that the infection is conveyed to the fœtus by the placental circulation. In the case of a syphilitic father, it is commonly believed that the infection is conveyed to the ovum through the seminal fluid at the moment of conception. If a series of children, one after the other, suffer from inherited syphilis, it is almost invariably the case that the mother has been infected.
In contrast to the acquired form, inherited syphilis is remarkable for the absence of any primary stage, the infection being a general one from the outset. The spirochæte is demonstrated in incredible numbers in the liver, spleen, lung, and other organs, and in the nasal secretion, and, from any of these, successful inoculations in monkeys can readily be made. The manifestations differ in degree rather than in kind from those of the acquired disease; the difference is partly due to the fact that the virus is attacking developing instead of fully formed tissues.
The virus exercises an injurious influence on the fœtus, which in many cases dies during the early months of intra-uterine life, so that miscarriage results, and this may take place in repeated pregnancies, the date at which the miscarriage occurs becoming later as the virus in the mother becomes attenuated. Eventually a child is carried to full term, and it may be still-born, or, if born alive, may suffer from syphilitic manifestations. It is difficult to explain such vagaries of syphilitic inheritance as the infection of one twin and the escape of the other.
Clinical Features.—We are not here concerned with the severe forms of the disease which prove fatal, but with the milder forms in which the infant is apparently healthy when born, but after from two to six weeks begins to show evidence of the syphilitic taint.
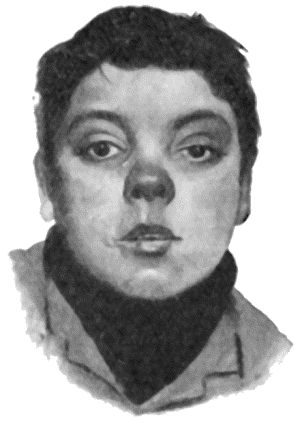
The usual phenomena are that the child ceases to thrive, becomes thin and sallow, and suffers from eruptions on the skin and mucous membranes. There is frequently a condition known as snuffles, in which the nasal passages are obstructed by an accumulation of thin muco-purulent discharge which causes the breathing to be noisy. It usually begins within a month after birth and before the eruptions on the skin appear. When long continued it is liable to interfere with the development of the nasal bones, so that when the child grows up there results a condition known as the “saddle-nose” deformity (Figs. 43 and 44).
Affections of the Skin.—Although all types of skin affection are met with in the inherited disease, the most important is a papular eruption, the papules being of large size, with a smooth shining top and of a reddish-brown colour. It affects chiefly the buttocks and thighs, the genitals, and other parts which are constantly moist. It is necessary to distinguish this specific eruption from a form of eczema which occurs in these situations in non-syphilitic children, the points that characterise the syphilitic condition being the infiltration of the skin and the coppery colour of the eruption. At the anus the papules acquire the characters of condylomata, also at the angles of the mouth, where they often ulcerate and leave radiating scars.
Affections of the Mucous Membranes.—The inflammation of the nasal mucous membrane that causes snuffles has already been referred to. There may be mucous patches in the mouth, or a stomatitis which is of importance, because it results in interference with the development of the permanent teeth. The mucous membrane of the larynx may be the seat of mucous patches or of catarrh, and as a result the child's cry is hoarse.
Affections of the Bones.—Swellings at the ends of the long bones, due to inflammation at the epiphysial junctions, are most often observed at the upper end of the humerus and in the bones in the region of the elbow. Partial displacement and mobility at the ossifying junction may be observed. The infant cries when the part is touched; and as it does not move the limb voluntarily, the condition is spoken of as the pseudo-paralysis of syphilis. Recovery takes place under anti-syphilitic treatment and immobilisation of the limb.
Diffuse thickening of the shafts of the long bones, due to a deposit of new bone by the periosteum, is sometimes met with.
The conditions of the skull known as Parrot's nodes or bosses, and craniotabes, were formerly believed to be characteristic of inherited syphilis, but they are now known to occur, particularly in rickety children, from other causes. The bosses result from the heaping up of new spongy bone beneath the pericranium, and they may be grouped symmetrically around the anterior fontanelle, or may extend along either side of the sagittal suture, which appears as a deep groove—the “natiform skull.” The bosses disappear in time, but the skull may remain permanently altered in shape, the frontal and parietal eminences appearing unduly prominent. The term craniotabes is applied when the bone becomes thin and soft, reverting to its original membranous condition, so that the affected areas dimple under the finger like parchment or thin cardboard; its localisation in the posterior parts of the skull suggests that the disappearance of the osseous tissue is influenced by the pressure of the head on the pillow. Craniotabes is recovered from as the child improves in health.
Between the ages of three and six months, certain other phenomena may be met with, such as effusion into the joints, especially the knees; iritis, in one or in both eyes, and enlargement of the spleen and liver.
In the majority of cases the child recovers from these early manifestations, especially when efficiently treated, and may enjoy an indefinite period of good health. On the other hand, when it attains the age of from two to four years, it may begin to manifest lesions which correspond to those of the tertiary period of acquired syphilis.
Later Lesions.—In the skin and subcutaneous tissue, the later manifestations may take the form of localised gummata, which tend to break down and form ulcers, on the leg for example, or of a spreading gummatous infiltration which is also liable to ulcerate, leaving disfiguring scars, especially on the face. The palate and fauces may be destroyed by ulceration. In the nose, especially when the ulcerative process is associated with a putrid discharge—ozæna—the destruction of tissue may be considerable and result in unsightly deformity. The entire palatal portions of the upper jaws, the vomer, turbinate, and other bones bounding the nasal and oral cavities, may disappear, so that on looking into the mouth the base of the skull is readily seen. Gummatous disease is frequently observed also in the flat bones of the skull, in the bones of the hand, as syphilitic dactylitis, and in the bones of the forearm and leg. When the tibia is affected the disease is frequently bilateral, and may assume the form of gummatous ulcers and sinuses. In later years the tibia may present alterations in shape resulting from antecedent gummatous disease—for example, nodular thickenings of the shaft, flattening of the crest, or a more uniform increase in thickness and length of the shaft of the bone, which, when it is curved in addition, is described as the “sabre-blade” deformity. Among lesions of the viscera, mention should be made of gumma of the testis, which causes the organ to become enlarged, uneven, and indurated. This has even been observed in infants a few months old.
Occasionally a syphilitic child suffers from a succession of these gummatous lesions with resulting ill-health, and, it may be, waxy disease of the internal organs; on the other hand, it may recover and present no further manifestations of the inherited taint.
Affections of the Eyes.—At or near puberty there is frequently observed an affection of the eyes, known as chronic interstitial keratitis, the relationship of which to inherited syphilis was first established by Hutchinson. It occurs between the ages of six and sixteen years, and usually affects one eye before the other. It commences as a diffuse haziness or steaminess near the centre of the cornea, and as it spreads the entire cornea assumes the appearance of ground glass. The chief complaint is of dimness of sight, which may almost amount to blindness, but there is little pain or photophobia; a certain amount of conjunctival and ciliary congestion is usually present, and there may be iritis in addition. The cornea, or parts of it, may become of a deep pink or salmon colour from the formation in it of new blood vessels. The affection may last for from eighteen months to two years. Complete recovery usually takes place, but slight opacities, especially in the site of former salmon patches, may persist, and the disease occasionally relapses. Choroiditis and retinitis may also occur, and leave permanent changes easily recognised on examination with the ophthalmoscope.
Among the rarer and more serious lesions of the inherited disease may be mentioned gummatous disease in the larynx and trachea, attended with ulceration and resulting in stenosis; and lesions of the nervous system which may result in convulsions, paralysis, or dementia.
In a limited number of cases, about the period of puberty there may develop deafness, which is usually bilateral and may become absolute.
Changes in the Permanent Teeth.—These affect specially the upper central incisors, which are dwarfed and stand somewhat apart in the gum, with their free edges converging towards one another. They are tapering or peg-shaped, and present at their cutting margin a deep semilunar notch. These appearances are commonly associated with the name of Hutchinson, who first described them. Affecting as they do the permanent teeth, they are not available for diagnosis until the child is over eight years of age. Henry Moon drew attention to a change in the first molars; these are reduced in size and dome-shaped through dwarfing of the central tubercle of each cusp.
Diagnosis of Inherited Syphilis.—When there is a typical eruption on the buttocks and snuffles there is no difficulty in recognising the disease. When, however, the rash is scanty or is obscured by co-existing eczema, most reliance should be placed on the distribution of the eruption, on the brown stains which are left after it has passed off, on the presence of condylomata, and of fissuring and scarring at the angles of the mouth. The history of the mother relative to repeated miscarriages and still-born children may afford confirmatory evidence. In doubtful cases, the diagnosis may be aided by the Wassermann test and by noting the therapeutic effects of grey powder, which, in syphilitic infants, usually effects a marked and rapid improvement both in the symptoms and in the general health.
While a considerable number of syphilitic children grow up without showing any trace of their syphilitic inheritance, the majority retain throughout life one or more of the following characteristics, which may therefore be described as permanent signs of the inherited disease: Dwarfing of stature from interference with growth at the epiphysial junctions; the forehead low and vertical, and the parietal and frontal eminences unduly prominent; the bridge of the nose sunken and rounded; radiating scars at the angles of the mouth; perforation or destruction of the hard palate; Hutchinson's teeth; opacities of the cornea from antecedent keratitis; alterations in the fundus oculi from choroiditis; deafness; depressed scars or nodes on the bones from previous gummata; “sabre-blade” or other deformity of the tibiæ.
The Contagiousness of Inherited Syphilis.—In 1837, Colles of Dublin stated his belief that, while a syphilitic infant may convey the disease to a healthy wet nurse, it is incapable of infecting its own mother if nursed by her, even although she may never have shown symptoms of the disease. This doctrine, which is known as Colles' law, is generally accepted in spite of the alleged occurrence of occasional exceptions. The older the child, the less risk there is of its communicating the disease to others, until eventually the tendency dies out altogether, as it does in the tertiary period of acquired syphilis. It should be added, however, that the contagiousness of inherited syphilis is denied by some observers, who affirm that, when syphilitic infants prove infective, the disease has been really acquired at or soon after birth.
There is general agreement that the subjects of inherited syphilis cannot transmit the disease by inheritance to their offspring, and that, although they very rarely acquire the disease de novo, it is possible for them to do so.
Prognosis of Inherited Syphilis.—Although inherited syphilis is responsible for a large but apparently diminishing mortality in infancy, the subjects of this disease may grow up to be as strong and healthy as their neighbours. Hutchinson insisted on the fact that there is little bad health in the general community that can be attributed to inherited syphilis.
Treatment.—Arsenical injections are as beneficial in the inherited as in the acquired disease. An infant the subject of inherited syphilis should, if possible, be nursed by its mother, and failing this it should be fed by hand. In infants at the breast, the drug may be given to the mother; in others, it is administered in the same manner as already described—only in smaller doses. On the first appearance of syphilitic manifestations it should be given 0.05 grm, novarsenbillon, injected into the deep subcutaneous tissues every week for six weeks, followed by one year's mercurial inunction—a piece of mercurial ointment the size of a pea being inserted under the infant's binder. In older children the dose is proportionately increased. The general health should be improved in every possible direction; considerable benefit may be derived from the use of cod-liver oil, and from preparations containing iron and calcium. Surgical interference may be required in the destructive gummatous lesions of the nose, throat, larynx, and bones, either with the object of arresting the spread of the disease, or of removing or alleviating the resulting deformities. In children suffering from keratitis, the eyes should be protected from the light by smoked or coloured glasses, and the pupils should be dilated with atropin from time to time, especially in cases complicated with iritis.
Acquired Syphilis in Infants and Young Children.—When syphilis is met with in infants and young children, it is apt to be taken for granted that the disease has been inherited. It is possible, however, for them to acquire the disease—as, for example, while passing through the maternal passages during birth, through being nursed or kissed by infected women, or through the rite of circumcision. The risk of infection which formerly existed by the arm-to-arm method of vaccination has been abolished by the use of calf lymph.
The clinical features of the acquired disease in infants and young children are similar to those observed in the adult, with a tendency, however, to be more severe, probably because the disease is often late in being recognised and treated.