
Fig. 38.—Primary Lesion on Thumb, with Secondary Eruption on Forearm.[1]
In the vast majority of cases, infection takes place during the congress of the sexes. Delicate, easily abraded surfaces are then brought into contact, and the discharge from lesions containing the virus is placed under favourable conditions for conveying the disease from one person to the other. In the male the possibility of infection taking place is increased if the virus is retained under cover of a long and tight prepuce, and if there are abrasions on the surface with which it comes in contact. The frequency with which infection takes place on the genitals during sexual intercourse warrants syphilis being considered a venereal disease, although there are other ways in which it may be contracted.
Some of these imply direct contact—such, for example, as kissing, the digital examination of syphilitic patients by doctors or nurses, or infection of the surgeon's fingers while operating upon a syphilitic patient. In suckling, a syphilitic wet nurse may infect a healthy infant, or a syphilitic infant may infect a healthy wet nurse. In other cases the infection is by indirect contact, the virus being conveyed through the medium of articles contaminated by a syphilitic patient—such, for example, as surgical instruments, tobacco pipes, wind instruments, table utensils, towels, or underclothing. Physiological secretions, such as saliva, milk, or tears, are not capable of communicating the disease unless contaminated by discharge from a syphilitic sore. While the saliva itself is innocuous, it can be, and often is, contaminated by the discharge from mucous patches or other syphilitic lesions in the mouth and throat, and is then a dangerous medium of infection. Unless these extra-genital sources of infection are borne in mind, there is a danger of failing to recognise the primary lesion of syphilis in unusual positions, such as the lip, finger, or nipple. When the disease is thus acquired by innocent transfer, it is known as syphilis insontium.
Stages or Periods of Syphilis.—Following the teaching of Ricord, it is customary to divide the life-history of syphilis into three periods or stages, referred to, for convenience, as primary, secondary, and tertiary. This division is to some extent arbitrary and artificial, as the different stages overlap one another, and the lesions of one stage merge insensibly into those of another. Wide variations are met with in the manifestations of the secondary stage, and histologically there is no valid distinction to be drawn between secondary and tertiary lesions.
The primary period embraces the interval that elapses between the initial infection and the first constitutional manifestations,—roughly, from four to eight weeks,—and includes the period of incubation, the development of the primary sore, and the enlargement of the nearest lymph glands.
The secondary period varies in duration from one to two years, during which time the patient is liable to suffer from manifestations which are for the most part superficial in character, affecting the skin and its appendages, the mucous membranes, and the lymph glands.
The tertiary period has no time-limit except that it follows upon the secondary, so that during the remainder of his life the patient is liable to suffer from manifestations which may affect the deeper tissues and internal organs as well as the skin and mucous membranes.
Primary Syphilis.—The period of incubation represents the interval that elapses between the occurrence of infection and the appearance of the primary lesion at the site of inoculation. Its limits may be stated as varying from two to six weeks, with an average of from twenty-one to twenty-eight days. While the disease is incubating, there is nothing to show that infection has occurred.
The Primary Lesion.—The incubation period having elapsed, there appears at the site of inoculation a circumscribed area of infiltration which represents the reaction of the tissues to the entrance of the virus. The first appearance is that of a sharply defined papule, rarely larger than a split pea. Its surface is at first smooth and shiny, but as necrosis of the tissue elements takes place in the centre, it becomes concave, and in many cases the epithelium is shed, and an ulcer is formed. Such an ulcer has an elevated border, sharply cut edges, an indurated base, and exudes a scanty serous discharge; its surface is at first occupied by yellow necrosed tissue, but in time this is replaced by smooth, pale-pink granulation tissue; finally, epithelium may spread over the surface, and the ulcer heals. As a rule, the patient suffers little discomfort, and may even be ignorant of the existence of the lesion, unless, as a result of exposure to mechanical or septic irritation, ulceration ensues, and the sore becomes painful and tender, and yields a purulent discharge. The primary lesion may persist until the secondary manifestations make their appearance, that is, for several weeks.
It cannot be emphasised too strongly that the induration of the primary lesion, which has obtained for it the name of “hard chancre,” is its most important characteristic. It is best appreciated when the sore is grasped from side to side between the finger and thumb. The sensation on grasping it has been aptly compared to that imparted by a nodule of cartilage, or by a button felt through a layer of cloth. The evidence obtained by touch is more valuable than that obtained by inspection, a fact which is made use of in the recognition of concealed chancres—that is, those which are hidden by a tight prepuce. The induration is due not only to the dense packing of the connective-tissue spaces with lymphocytes and plasma cells, but also to the formation of new connective-tissue elements. It is most marked in chancres situated in the furrow between the glans and the prepuce.
In the male, the primary lesion specially affects certain situations, and the appearances vary with these: (1) On the inner aspect of the prepuce, and in the fold between the prepuce and the glans; in the latter situation the induration imparts a “collar-like” rigidity to the prepuce, which is most apparent when it is rolled back over the corona. (2) At the orifice of the prepuce the primary lesion assumes the form of multiple linear ulcers or fissures, and as each of these is attended with infiltration, the prepuce cannot be pulled back—a condition known as syphilitic phimosis. (3) On the glans penis the infiltration may be so superficial that it resembles a layer of parchment, but if it invades the cavernous tissue there is a dense mass of induration. (4) On the external aspect of the prepuce or on the skin of the penis itself. (5) At either end of the torn frænum, in the form of a diamond-shaped ulcer raised above the surroundings. (6) In relation to the meatus and canal of the urethra, in either of which situations the swelling and induration may lead to narrowing of the urethra, so that the urine is passed with pain and difficulty and in a minute stream; stricture results only in the exceptional cases in which the chancre has ulcerated and caused destruction of tissue. A chancre within the orifice of the urethra is rare, and, being concealed from view, it can only be recognised by the discharge from the meatus and by the induration felt between the finger and thumb on palpating the urethra.
In the female, the primary lesion is not so typical or so easily recognised as in men; it is usually met with on the labia; the induration is rarely characteristic and does not last so long. The primary lesion may take the form of condylomata. Indurated œdema, with brownish-red or livid discoloration of one or both labia, is diagnostic of syphilis.
The hard chancre is usually solitary, but sometimes there are two or more; when there are several, they are individually smaller than the solitary chancre.
It is the exception for a hard chancre to leave a visible scar, hence, in examining patients with a doubtful history of syphilis, little reliance can be placed on the presence or absence of a scar on the genitals. When the primary lesion has taken the form of an open ulcer with purulent discharge, or has sloughed, there is a permanent scar.
Infection of the adjacent lymph glands is usually found to have taken place by the time the primary lesion has acquired its characteristic induration. Several of the glands along Poupart's ligament, on one or on both sides, become enlarged, rounded, and indurated; they are usually freely movable, and are rarely sensitive unless there is superadded septic infection. The term bullet-bubo has been applied to them, and their presence is of great value in diagnosis. In a certain number of cases, one of the main lymph vessels on the dorsum of the penis is transformed into a fibrous cord easily recognisable on palpation, and when grasped between the fingers appears to be in size and consistence not unlike the vas deferens.
Concealed chancre is the term applied when one or more chancres are situated within the sac of a prepuce which cannot be retracted. If the induration is well marked, the chancre can be palpated through the prepuce, and is tender on pressure. As under these conditions it is impossible for the patient to keep the parts clean, septic infection becomes a prominent feature, the prepuce is œdematous and inflamed, and there is an abundant discharge of pus from its orifice. It occasionally happens that the infection assumes a virulent character and causes sloughing of the prepuce—a condition known as phagedæna. The discharge is then foul and blood-stained, and the prepuce becomes of a dusky red or purple colour, and may finally slough, exposing the glans.
Extra-genital or Erratic Chancres (Fig. 38).—Erratic chancre is the term applied by Jonathan Hutchinson to the primary lesion of syphilis when it appears on parts of the body other than the genitals. It differs in some respects from the hard chancre as met with on the penis; it is usually larger, the induration is more diffused, and the enlarged glands are softer and more sensitive. The glands in nearest relation to the sore are those first affected, for example, the epitrochlear or axillary glands in chancre of the finger; the submaxillary glands in chancre of the lip or mouth; or the pre-auricular gland in chancre of the eyelid or forehead. In consequence of their divergence from the typical chancre, and of their being often met with in persons who, from age, surroundings, or moral character, are unlikely subjects of venereal disease, the true nature of erratic chancres is often overlooked until the persistence of the lesion, its want of resemblance to anything else, or the onset of constitutional symptoms, determines the diagnosis of syphilis. A solitary, indolent sore occurring on the lip, eyelid, finger, or nipple, which does not heal but tends to increase in size, and is associated with induration and enlargement of the adjacent glands, is most likely to be the primary lesion of syphilis.
[1] From A System of Syphilis, vol. ii., edited by D'Arcy Power and J. Keogh Murphy, Oxford Medical Publications.
The Soft Sore, Soft Chancre, or Chancroid.—The differential diagnosis of syphilis necessitates the consideration of the soft sore, soft chancre, or chancroid, which is also a common form of venereal disease, and is due to infection with a virulent pus-forming bacillus, first described by Ducrey in 1889. Ducrey's bacillus occurs in the form of minute oval rods measuring about 1.5 µ in length, which stain readily with any basic aniline dye, but are quickly decolorised by Gram's method. They are found mixed with other organisms in the purulent discharge from the sore, and are chiefly arranged in small groups or in short chains. Soft sores are always contracted by direct contact from another individual, and the incubation period is a short one of from two to five days. They are usually situated in the vicinity of the frænum, and, in women, about the labia minora or fourchette; they probably originate in abrasions in these situations. They appear as pustules, which are rapidly converted into small, acutely inflamed ulcers with sharply cut, irregular margins, which bleed easily and yield an abundant yellow purulent discharge. They are devoid of the induration of syphilis, are painful, and nearly always multiple, reproducing themselves in successive crops by auto-inoculation. Soft sores are often complicated by phimosis and balanitis, and they frequently lead to infection of the glands in the groin. The resulting bubo is ill-defined, painful, and tender, and suppuration occurs in about one-fourth of the cases. The overlying skin becomes adherent and red, and suppuration takes place either in the form of separate foci in the interior of the individual glands, or around them; in the latter case, on incision, the glands are found lying bathed in pus. Ducrey's bacillus is found in pure culture in the pus. Sometimes other pyogenic organisms are superadded. After the bubo has been opened the wound may take on the characters of a soft sore.
Treatment.—Soft sores heal rapidly when kept clean. If concealed under a tight prepuce, an incision should be made along the dorsum to give access to the sores. They should be washed with eusol, and dusted with a mixture of one part iodoform and two parts boracic or salicylic acid, or, when the odour of iodoform is objected to, of equal parts of boracic acid and carbonate of zinc. Immersion of the penis in a bath of eusol for some hours daily is useful. The sore is then covered with a piece of gauze kept in position by drawing the prepuce over it, or by a few turns of a narrow bandage. Sublimed sulphur frequently rubbed into the sore is recommended by C. H. Mills. If the sores spread in spite of this, they should be painted with cocaine and then cauterised. When the glands in the groin are infected, the patient must be confined to bed, and a dressing impregnated with ichthyol and glycerin (10 per cent.) applied; the repeated use of a suction bell is of great service. Harrison recommends aspiration of a bubonic abscess, followed by injection of 1 in 20 solution of tincture of iodine into the cavity; this is in turn aspirated, and then 1 or 2 c.c. of the solution injected and left in. This is repeated as often as the cavity refills. It is sometimes necessary to let the pus out by one or more small incisions and continue the use of the suction bell.
Diagnosis of Primary Syphilis.—In cases in which there is a history of an incubation period of from three to five weeks, when the sore is indurated, persistent, and indolent, and attended with bullet-buboes in the groin, the diagnosis of primary syphilis is not difficult. Owing, however, to the great importance of instituting treatment at the earliest possible stage of the infection, an effort should be made to establish the diagnosis without delay by demonstrating the spirochæte. Before any antiseptic is applied, the margin of the suspected sore is rubbed with gauze, and the serum that exudes on pressure is collected in a capillary tube and sent to a pathologist for microscopical examination. A better specimen can sometimes be obtained by puncturing an enlarged lymph gland with a hypodermic needle, injecting a few minims of sterile saline solution and then aspirating the blood-stained fluid.
The Wassermann test must not be relied upon for diagnosis in the early stage, as it does not appear until the disease has become generalised and the secondary manifestations are about to begin. The practice of waiting in doubtful cases before making a diagnosis until secondary manifestations appear is to be condemned.
Extra-genital chancres, e.g. sores on the fingers of doctors or nurses, are specially liable to be overlooked, if the possibility of syphilis is not kept in mind.
It is important to bear in mind the possibility of a patient having acquired a mixed infection with the virus of soft chancre, which will manifest itself a few days after infection, and the virus of syphilis, which shows itself after an interval of several weeks. This occurrence was formerly the source of much confusion in diagnosis, and it was believed at one time that syphilis might result from soft sores, but it is now established that syphilis does not follow upon soft sores unless the virus of syphilis has been introduced at the same time. The practitioner must be on his guard, therefore, when a patient asks his advice concerning a venereal sore which has appeared within a few days of exposure to infection. Such a patient is naturally anxious to know whether he has contracted syphilis or not, but neither a positive nor a negative answer can be given—unless the spirochæte can be identified.
Syphilis is also to be diagnosed from epithelioma, the common form of cancer of the penis. It is especially in elderly patients with a tight prepuce that the induration of syphilis is liable to be mistaken for that associated with epithelioma. In difficult cases the prepuce must be slit open.
Difficulty may occur in the diagnosis of primary syphilis from herpes, as this may appear as late as ten days after connection; it commences as a group of vesicles which soon burst and leave shallow ulcers with a yellow floor; these disappear quickly on the use of an antiseptic dusting powder.
Apprehensive patients who have committed sexual indiscretions are apt to regard as syphilitic any lesion which happens to be located on the penis—for example, acne pustules, eczema, psoriasis papules, boils, balanitis, or venereal warts.
The local treatment of the primary sore consists in attempting to destroy the organisms in situ. An ointment made up of calomel 33 parts, lanoline 67 parts, and vaseline 10 parts (Metchnikoff's cream) is rubbed into the sore several times a day. If the surface is unbroken, it may be dusted lightly with a powder composed of equal parts of calomel and carbonate of zinc. A gauze dressing is applied, and the penis and scrotum should be supported against the abdominal wall by a triangular handkerchief or bathing-drawers; if there is inflammatory œdema the patient should be confined to bed.
In concealed chancres with phimosis, the sac of the prepuce should be slit up along the dorsum to admit of the ointment being applied. If phagedæna occurs, the prepuce must be slit open along the dorsum, or if sloughing, cut away, and the patient should have frequent sitz baths of weak sublimate lotion. When the chancre is within the meatus, iodoform bougies are inserted into the urethra, and the urine should be rendered bland by drinking large quantities of fluid.
General treatment is considered on p. 149.
Secondary Syphilis.—The following description of secondary syphilis is based on the average course of the disease in untreated cases. The onset of constitutional symptoms occurs from six to twelve weeks after infection, and the manifestations are the result of the entrance of the virus into the general circulation, and its being carried to all parts of the body. The period during which the patient is liable to suffer from secondary symptoms ranges from six months to two years.
In some cases the general health is not disturbed; in others the patient is feverish and out of sorts, losing appetite, becoming pale and anæmic, complaining of lassitude, incapacity for exertion, headache, and pains of a rheumatic type referred to the bones. There is a moderate degree of leucocytosis, but the increase is due not to the polymorpho-nuclear leucocytes but to lymphocytes. In isolated cases the temperature rises to 101° or 102° F. and the patient loses flesh. The lymph glands, particularly those along the posterior border of the sterno-mastoid, become enlarged and slightly tender. The hair comes out, eruptions appear on the skin and mucous membranes, and the patient may suffer from sore throat and affections of the eyes. The local lesions are to be regarded as being of the nature of reactions against accumulations of the parasite, lymphocytes and plasma cells being the elements chiefly concerned in the reactive process.
Affections of the Skin are among the most constant manifestations. An evanescent macular rash, not unlike that of measles—roseola—is the first to appear, usually in from six to eight weeks from the date of infection; it is widely diffused over the trunk, and the original dull rose-colour soon fades, leaving brownish stains, which in time disappear. It is usually followed by a papular eruption, the individual papules being raised above the surface of the skin, smooth or scaly, and as they are due to infiltration of the skin they are more persistent than the roseoles. They vary in size and distribution, being sometimes small, hard, polished, and closely aggregated like lichen, sometimes as large as a shilling-piece, with an accumulation of scales on the surface like that seen in psoriasis. The co-existence of scaly papules and faded roseoles is very suggestive of syphilis.
Other types of eruption are less common, and are met with from the third month onwards. A pustular eruption, not unlike that of acne, is sometimes a prominent feature, but is not characteristic of syphilis unless it affects the scalp and forehead and is associated with the remains of the papular eruption. The term ecthyma is applied when the pustules are of large size, and, after breaking on the surface, give rise to superficial ulcers; the discharge from the ulcer often dries up and forms a scab or crust which is continually added to from below as the ulcer extends in area and depth. The term rupia is applied when the crusts are prominent, dark in colour, and conical in shape, roughly resembling the shell of a limpet. If the crust is detached, a sharply defined ulcer is exposed, and when this heals it leaves a scar which is usually circular, thin, white, shining like satin, and the surrounding skin is darkly pigmented; in the case of deep ulcers, the scar is depressed and adherent (Fig. 39).
In the later stages there may occur a form of creeping or spreading ulceration of the skin of the face, groin, or scrotum, healing at one edge and spreading at another like tuberculous lupus, but distinguished from this by its more rapid progress and by the pigmentation of the scar.
Condylomata are more characteristic of syphilis than any other type of skin lesion. They are papules occurring on those parts of the body where the skin is habitually moist, and especially where two skin surfaces are in contact. They are chiefly met with on the external genitals, especially in women, around the anus, beneath large pendulous mammæ, between the toes, and at the angles of the mouth, and in these situations their development is greatly favoured by neglect of cleanliness. They present the appearance of well-defined circular or ovoid areas in which the skin is thickened and raised above the surface; they are covered with a white sodden epidermis, and furnish a scanty but very infective discharge. Under the influence of irritation and want of rest, as at the anus or at the angle of the mouth, they are apt to become fissured and superficially ulcerated, and the discharge then becomes abundant and may crust on the surface, forming yellow scabs. At the angle of the mouth the condylomatous patches may spread to the cheek, and when they ulcerate may leave fissure-like scars radiating from the mouth—an appearance best seen in inherited syphilis (Fig. 44).
The Appendages of the Skin.—The hair loses its gloss, becomes dry and brittle, and readily falls out, either as an exaggeration of the normal shedding of the hair, or in scattered areas over the scalp (syphilitic alopœcia). The hair is not re-formed in the scars which result from ulcerated lesions of the scalp. The nail-folds occasionally present a pustular eruption and superficial ulceration, to which the name syphilitic onychia has been applied; more commonly the nails become brittle and ragged, and they may even be shed.
The Mucous Membranes, and especially those of the mouth and throat, suffer from lesions similar to those met with on the skin. On a mucous surface the papular eruption assumes the form of mucous patches, which are areas with a congested base covered with a thin white film of sodden epithelium like wet tissue-paper. They are best seen on the inner aspect of the cheeks, the soft palate, uvula, pillars of the fauces, and tonsils. In addition to mucous patches, there may be a number of small, superficial, kidney-shaped ulcers, especially along the margins of the tongue and on the tonsils. In the absence of mucous patches and ulcers, the sore throat may be characterised by a bluish tinge of the inflamed mucous membrane and a thin film of shed epithelium on the surface. Sometimes there is an elongated sinuous film which has been likened to the track of a snail. In the larynx the presence of congestion, œdema, and mucous patches may be the cause of persistent hoarseness. The tongue often presents a combination of lesions, including ulcers, patches where the papillæ are absent, fissures, and raised white papules resembling warts, especially towards the centre of the dorsum. These lesions are specially apt to occur in those who smoke, drink undiluted alcohol or spirits, or eat hot condiments to excess, or who have irregular, sharp-cornered teeth. At a later period, and in those who are broken down in health from intemperance or other cause, the sore throat may take the form of rapidly spreading, penetrating ulcers in the soft palate and pillars of the fauces, which may lead to extensive destruction of tissue, with subsequent scars and deformity highly characteristic of previous syphilis.
In the Bones, lesions occur which assume the clinical features of an evanescent periostitis, the patient complaining of nocturnal pains over the frontal bone, sternum, tibiæ, and ulnæ, and localised tenderness on tapping over these bones.
In the Joints, a serous synovitis or hydrops may occur, chiefly in the knee, on one or on both sides.
The Affections of the Eyes, although fortunately rare, are of great importance because of the serious results which may follow if they are not recognised and treated. Iritis is the commonest of these, and may occur in one or in both eyes, one after the other, from three to eight months after infection. The patient complains of impairment of sight and of frontal or supraorbital pain. The eye waters and is hypersensitive, the iris is discoloured and reacts sluggishly to light, and there is a zone of ciliary congestion around the cornea. The appearance of minute white nodules or flakes of lymph at the margin of the pupil is especially characteristic of syphilitic iritis. When adhesions have formed between the iris and the structures in relation to it, the pupil dilates irregularly under atropin. Although complete recovery is to be expected under early and energetic treatment, if neglected, iritis may result in occlusion of the pupil and permanent impairment or loss of sight.
The other lesions of the eye are much rarer, and can only be discovered on ophthalmoscopic examination.
The virus of syphilis exerts a special influence upon the Blood Vessels, exciting a proliferation of the endothelial lining which results in narrowing of their lumen, endarteritis, and a perivascular infiltration in the form of accumulations of plasma cells around the vessels and in the lymphatics that accompany them.
In the Brain, in the later periods of secondary and in tertiary syphilis, changes occur as a result of the narrowing of the lumen of the arteries, or of their complete obliteration by thrombosis. By interfering with the nutrition of those parts of the brain supplied by the affected arteries, these lesions give rise to clinical features of which severe headache and paralysis are the most prominent.
Affections of the Spinal Cord are extremely rare, but paraplegia from myelitis has been observed.
Lastly, attention must be directed to the remarkable variations observed in different patients. Sometimes the virulent character of the disease can only be accounted for by an idiosyncrasy of the patient. Constitutional symptoms, particularly pyrexia and anæmia, are most often met with in young women. Patients over forty years of age have greater difficulty in overcoming the infection than younger adults. Malarial and other infections, and the conditions attending life in tropical countries, from the debility which they cause, tend to aggravate and prolong the disease, which then assumes the characters of what has been called malignant syphilis. All chronic ailments have a similar influence, and alcoholic intemperance is universally regarded as a serious aggravating factor.
Diagnosis of Secondary Syphilis.—A routine examination should be made of the parts of the body which are most often affected in this disease—the scalp, mouth, throat, posterior cervical glands, and the trunk, the patient being stripped and examined by daylight. Among the diagnostic features of the skin affections the following may be mentioned: They are frequently, and sometimes to a marked degree, symmetrical; more than one type of eruption—papules and pustules, for example—are present at the same time; there is little itching; they are at first a dull-red colour, but later present a brown pigmentation which has been likened to the colour of raw ham; they exhibit a predilection for those parts of the forehead and neck which are close to the roots of the hair; they tend to pass off spontaneously; and they disappear rapidly under treatment.
Serum Diagnosis—Wassermann Reaction.—Wassermann found that if an extract of syphilitic liver rich in spirochætes is mixed with the serum from a syphilitic patient, a large amount of complement is fixed. The application of the test is highly complicated and can only be carried out by an expert pathologist. For the purpose he is supplied with from 5 c.c. to 10 c.c. of the patient's blood, withdrawn under aseptic conditions from the median basilic vein by means of a serum syringe, and transferred to a clean and dry glass tube. There is abundant evidence that the Wassermann test is a reliable means of establishing a diagnosis of syphilis.
A definitely positive reaction can usually be obtained between the fifteenth and thirtieth day after the appearance of the primary lesion, and as time goes on it becomes more marked. During the secondary period the reaction is practically always positive. In the tertiary stage also it is positive except in so far as it is modified by the results of treatment. In para-syphilitic lesions such as general paralysis and tabes a positive reaction is almost always present. In inherited syphilis the reaction is positive in every case. A positive reaction may be present in other diseases, for example, frambesia, trypanosomiasis, and leprosy.
As the presence of the reaction is an evidence of the activity of the spirochætes, repeated applications of the test furnish a valuable means of estimating the efficacy of treatment. The object aimed at is to change a persistently positive reaction to a permanently negative one.
Treatment of Syphilis.—In the treatment of syphilis the two main objects are to maintain the general health at the highest possible standard, and to introduce into the system therapeutic agents which will inhibit or destroy the invading parasite.
The second of these objects has been achieved by the researches of Ehrlich, who, in conjunction with his pupil, Hata, has built up a compound, the dihydrochloride of dioxydiamido-arseno-benzol, popularly known as salvarsan or “606.” Other preparations, such as kharsivan, arseno-billon, and diarsenol, are chemically equivalent to salvarsan, containing from 27 to 31 per cent. of arsenic, and are equally efficient. The full dose is 0.6 grm. All these members of the “606” group form an acid solution when dissolved in water, and must be rendered alkaline before being injected. As subcutaneous and intra-muscular injections cause considerable pain, and may cause sloughing of the tissues, “606” preparations must be injected intravenously. Ehrlich has devised a preparation—neo-salvarsan, or “914,” which is more easily prepared and forms a neutral solution. It contains from 18 to 20 per cent. of arsenic. Neo-kharsivan, novo-arseno-billon, and neo-diarsenol belong to the “914” group, the full dosage of which is 0.9 grm. As subcutaneous and intra-muscular injections of the “914” group are not painful, and even more efficient than intravenous injections, the administration is simpler.
Galyl, luargol, and other preparations act in the same way as the “606” and “914” groups.
The “606” preparations may be introduced into the veins by injection or by means of an apparatus which allows the solution to flow in by gravity. The left median basilic vein is selected, and a platino-iridium needle with a short point and a bore larger than that of the ordinary hypodermic syringe is used. The needle is passed for a few millimetres along the vein, and the solution is then slowly introduced; before withdrawing the needle some saline is run in to diminish the risk of thrombosis.
The “914” preparations may be injected either into the subcutaneous tissue of the buttock or into the substance of the gluteus muscle. The part is then massaged for a few minutes, and the massage is repeated daily for a few days.
No hard-and-fast rules can be laid down as to what constitutes a complete course of treatment. Harrison recommends as a minimum course of one of the “914” preparations in early primary cases an initial dose of 0.45 grm. given intra-muscularly or into the deep subcutaneous tissue; the same dose a week later; 0.6 grm. the following week; then miss a week and give 9.6 grms. on two successive weeks; then miss two weeks and give 0.6 grm. on two more successive weeks.
When a positive Wassermann reaction is present before treatment is commenced, the above course is prolonged as follows: for three weeks is given a course of potassium iodide, after which four more weekly injections of 0.6 grm. of “914” are given.
With each injection of “914” after the first, throughout the whole course 1 grain of mercury is injected intra-muscularly.
In the course of a few hours, there is usually some indisposition, with a feeling of chilliness and slight rise of temperature; these symptoms pass off within twenty-four hours, and in a few days there is a decided improvement of health. Three or four days after an intra-muscular injection there may be pain and stiffness in the gluteal region.
These preparations are the most efficient therapeutic agents that have yet been employed in the treatment of syphilis.
The manifestations of the disease disappear with remarkable rapidity. Observations show that the spirochætes lose their capacity for movement within an hour or two of the administration, and usually disappear altogether in from twenty-four to thirty-six hours. Wassermann's reaction usually yields a negative result in from three weeks to two months, but later may again become positive. Subsequent doses of the arsenical preparation are therefore usually indicated, and should be given in from 7 to 21 days according to the dose.
When syphilis occurs in a pregnant woman, she should be given in the early months an ordinary course of “914,” followed by 10-grain doses of potassium iodide twice daily. The injections may be repeated two months later, and during the remainder of the pregnancy 2-grain mercury pills are given twice daily (A. Campbell). The presence of albumen in the urine contra-indicates arsenical treatment.
It need scarcely be pointed out that the use of powerful drugs like “606” and “914” is not free from risk; it may be mentioned that each dose contains nearly three grains of arsenic. Before the administration the patient must be overhauled; its administration is contra-indicated in the presence of disease of the heart and blood vessels, especially a combination of syphilitic aortitis and sclerosis of the coronary arteries, with degeneration of the heart muscle; in affections of the central nervous system, especially advanced paralysis, and in such disturbances of metabolism as are associated with diabetes and Bright's disease. Its use is not contra-indicated in any lesion of active syphilis.
The administration is controlled by the systematic examination of the urine for arsenic.
The Administration of Mercury.—The success of the arsenical preparations has diminished the importance of mercury in the treatment of syphilis, but it is still used to supplement the effect of the injections. The amount of mercury to be given in any case must be proportioned to the idiosyncrasies of the patient, and it is advisable, before commencing the treatment, to test his urine and record his body-weight. The small amount of mercury given at the outset is gradually increased. If the body-weight falls, or if the gums become sore and the breath foul, the mercury should be stopped for a time. If salivation occurs, the drinking of hot water and the taking of hot baths should be insisted upon, and half-dram doses of the alkaline sulphates prescribed.
Methods of Administering Mercury.—(1) By the Mouth.—This was for long the most popular method in this country, the preparation usually employed being grey powder, in pills or tablets, each of which contains one grain of the powder. Three of these are given daily in the first instance, and the daily dose is increased to five or even seven grains till the standard for the individual patient is arrived at. As the grey powder alone sometimes causes irritation of the bowels, it should be combined with iron, as in the following formula: Hydrarg. c. cret. gr. 1; ferri sulph. exsiccat. gr. 1 or 2.
(2) By Inunction.—Inunction consists in rubbing into the pores of the skin an ointment composed of equal parts of 20 per cent. oleate of mercury and lanolin. Every night after a hot bath, a dram of the ointment (made up by the chemist in paper packets) is rubbed for fifteen minutes into the skin where it is soft and comparatively free from hairs. When the patient has been brought under the influence of the mercury, inunction may be replaced by one of the other methods, of administering the drug.
(3) By Intra-muscular Injection.—This consists in introducing the drug by means of a hypodermic syringe into the substance of the gluteal muscles. The syringe is made of glass, and has a solid glass piston; the needle of platino-iridium should be 5 cm. long and of a larger calibre than the ordinary hypodermic needle. The preparation usually employed consists of: metallic mercury or calomel 1 dram, lanolin and olive oil each 2 drams; it must be warmed to allow of its passage through the needle. Five minims—containing one grain of metallic mercury—represent a dose, and this is injected into the muscles above and behind the great trochanter once a week. The contents of the syringe are slowly expressed, and, after withdrawing the needle, gentle massage of the buttock should be employed. Four courses each of ten injections are given the first year, three courses of the same number during the second and third years, and two courses during the fourth year (Lambkin).
The General Health.—The patient must lead a regular life and cultivate the fresh-air habit, which is as beneficial in syphilis as in tuberculosis. Anæmia, malaria, and other sources of debility must receive appropriate treatment. The diet should be simple and easily digested, and should include a full supply of milk. Alcohol is prohibited. The excretory organs are encouraged to act by the liberal drinking of hot water between meals, say five or six tumblerfuls in the twenty-four hours. The functions of the skin are further aided by frequent hot baths, and by the wearing of warm underclothing. While the patient should avoid exposure to cold, and taxing his energies by undue exertion, he should be advised to take exercise in the open air. On account of the liability to lesions of the mouth and throat, he should use tobacco in moderation, his teeth should be thoroughly overhauled by the dentist, and he should brush them after every meal, using an antiseptic tooth powder or wash. The mouth and throat should be rinsed out night and morning with a solution of chlorate of potash and alum, or with peroxide of hydrogen.
Treatment of the Local Manifestations.—The skin lesions are treated on the same lines as similar eruptions of other origin. As local applications, preparations of mercury are usually selected, notably the ointments of the red oxide of mercury, ammoniated mercury, or oleate of mercury (5 per cent.), or the mercurial plaster introduced by Unna. In the treatment of condylomata the greatest attention must be paid to cleanliness and dryness. After washing and drying the affected patches, they are dusted with a powder consisting of equal parts of calomel and carbonate of zinc; and apposed skin surfaces, such as the nates or labia, are separated by sublimate wool. In the ulcers of later secondary syphilis, crusts are got rid of in the first instance by means of a boracic poultice, after which a piece of lint or gauze cut to the size of the ulcer and soaked in black wash is applied and covered with oil-silk. If the ulcer tends to spread in area or in depth, it should be scraped with a sharp spoon, and painted over with acid nitrate of mercury, or a local hyperæmia may be induced by Klapp's suction apparatus.
In lesions of the mouth and throat, the teeth should be attended to; the best local application is a solution of chromic acid—10 grains to the ounce—painted on with a brush once daily. If this fails, the lesions may be dusted with calomel the last thing at night. For deep ulcers of the throat the patient should gargle frequently with chlorine water or with perchloride of mercury (1 in 2000); if the ulcer continues to spread it should be painted with acid nitrate of mercury.
In the treatment of iritis the eyes are shaded from the light and completely rested, and the pupil is well dilated by atropin to prevent adhesions. If there is much pain, a blister may be applied to the temple.
The Relations of Syphilis to Marriage.—Before the introduction of the Ehrlich-Hata treatment no patient was allowed to marry until three years had elapsed after the disappearance of the last manifestation. While marriage might be entered upon under these conditions without risk of the husband infecting the wife, the possibility of his conveying the disease to the offspring cannot be absolutely excluded. It is recommended, as a precautionary measure, to give a further mercurial course of two or three months' duration before marriage, and an intravenous injection of an arsenical preparation.
Intermediate Stage.—After the dying away of the secondary manifestations and before the appearance of tertiary lesions, the patient may present certain symptoms which Hutchinson called reminders. These usually consist of relapses of certain of the affections of the skin, mouth, or throat, already described. In the skin, they may assume the form of peeling patches in the palms, or may appear as spreading and confluent circles of a scaly papular eruption, which if neglected may lead to the formation of fissures and superficial ulcers. Less frequently there is a relapse of the eye affections, or of paralytic symptoms from disease of the cerebral arteries.
Tertiary Syphilis.—While the manifestations of primary and secondary syphilis are common, those of the tertiary period are by comparison rare, and are observed chiefly in those who have either neglected treatment or who have had their powers of resistance lowered by privation, by alcoholic indulgence, or by tropical disease.
It is to be borne in mind that in a certain proportion of men and in a larger proportion of women, the patient has no knowledge of having suffered from syphilis. Certain slight but important signs may give the clue in a number of cases, such as irregularity of the pupils or failure to react to light, abnormality of the reflexes, and the discovery of patches of leucoplakia on the tongue, cheek, or palate.
The general character of tertiary manifestations may be stated as follows: They attack by preference the tissues derived from the mesoblastic layer of the embryo—the cellular tissue, bones, muscles, and viscera. They are often localised to one particular tissue or organ, such, for example, as the subcutaneous cellular tissue, the bones, or the liver, and they are rarely symmetrical. They are usually aggressive and persistent, with little tendency to natural cure, and they may be dangerous to life, because of the destructive changes produced in such organs as the brain or the larynx. They are remarkably amenable to treatment if instituted before the stage which is attended with destruction of tissue is reached. Early tertiary lesions may be infective, and the disease may be transmitted by the discharges from them; but the later the lesions the less is the risk of their containing an infective virus.
The most prominent feature of tertiary syphilis consists in the formation of granulation tissue, and this takes place on a scale considerably larger than that observed in lesions of the secondary period. The granulation tissue frequently forms a definite swelling or tumour-like mass (syphiloma), which, from its peculiar elastic consistence, is known as a gumma. In its early stages a gumma is a firm, semi-translucent greyish or greyish-red mass of tissue; later it becomes opaque, yellow, and caseous, with a tendency to soften and liquefy. The gumma does harm by displacing and replacing the normal tissue elements of the part affected, and by involving these in the degenerative changes, of the nature of caseation and necrosis, which produce the destructive lesions of the skin, mucous membranes, and internal organs. This is true not only of the circumscribed gumma, but of the condition known as gummatous infiltration or syphilitic cirrhosis, in which the granulation tissue is diffused throughout the connective-tissue framework of such organs as the tongue or liver. Both the gummatous lesions and the fibrosis of tertiary syphilis are directly excited by the spirochætes.
The life-history of an untreated gumma varies with its environment. When protected from injury and irritation in the substance of an internal organ such as the liver, it may become encapsulated by fibrous tissue, and persist in this condition for an indefinite period, or it may be absorbed and leave in its place a fibrous cicatrix. In the interior of a long bone it may replace the rigid framework of the shaft to such an extent as to lead to pathological fracture. If it is near the surface of the body—as, for example, in the subcutaneous or submucous cellular tissue, or in the periosteum of a superficial bone, such as the palate, the skull, or the tibia—the tissue of which it is composed is apt to undergo necrosis, in which the overlying skin or mucous membrane frequently participates, the result being an ulcer—the tertiary syphilitic ulcer (Figs. 40 and 41).
Tertiary Lesions of the Skin and Subcutaneous Cellular Tissue.—The clinical features of a subcutaneous gumma are those of an indolent, painless, elastic swelling, varying in size from a pea to an almond or walnut. After a variable period it usually softens in the centre, the skin over it becomes livid and dusky, and finally separates as a slough, exposing the tissue of the gumma, which sometimes appears as a mucoid, yellowish, honey-like substance, more frequently as a sodden, caseated tissue resembling wash-leather. The caseated tissue of a gumma differs from that of a tuberculous lesion in being tough and firm, of a buff colour like wash-leather, or whitish, like boiled fish. The degenerated tissue separates slowly and gradually, and in untreated cases may be visible for weeks in the floor of the ulcer.
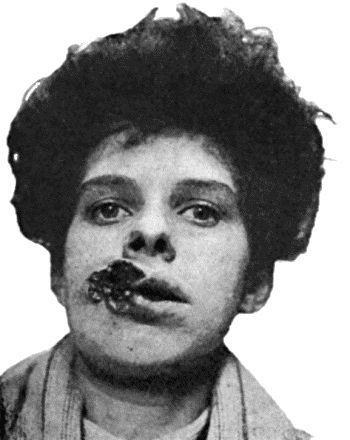
Fig. 40.—Ulcerating Gumma of Lips.
(From a photograph lent by Dr. Stopford Taylor and Dr. R. W. Mackenna.)
The tertiary ulcer may be situated anywhere, but is most frequently met with on the leg, especially in the region of the knee (Fig. 42) and over the calf. There may be one or more ulcers, and also scars of antecedent ulcers. The edges are sharply cut, as if punched out; the margins are rounded in outline, firm, and congested; the base is occupied by gummatous tissue, or, if this has already separated and sloughed out, by unhealthy granulations and a thick purulent discharge. When the ulcer has healed it leaves a scar which is depressed, and if over a bone, is adherent to it. The features of the tertiary ulcer, however, are not always so characteristic as the above description would imply. It is to be diagnosed from the “leg ulcer,” which occurs almost exclusively on the lower third of the leg; from Bazin's disease (p. 74); from the ulcers that result from certain forms of malignant disease, such as rodent cancer, and from those met with in chronic glanders.
Gummatous Infiltration of the Skin (“Syphilitic Lupus”).—This is a lesion, met with chiefly on the face and in the region of the external genitals, in which the skin becomes infiltrated with granulation tissue so that it is thickened, raised above the surface, and of a brownish-red colour. It appears as isolated nodules, which may fuse together; the epidermis becomes scaly and is shed, giving rise to superficial ulcers which are usually covered by crusted discharge. The disease tends to spread, creeping over the skin with a serpiginous, crescentic, or horse-shoe margin, while the central portion may heal and leave a scar. From the fact of its healing in the centre while it spreads at the margin, it may resemble tuberculous disease of the skin. It can usually be differentiated by observing that the infiltration is on a larger scale; the progress is much more rapid, involving in the course of months an area which in the case of tuberculosis would require as many years; the scars are sounder and are less liable to break down again; and the disease rapidly yields to anti-syphilitic treatment.
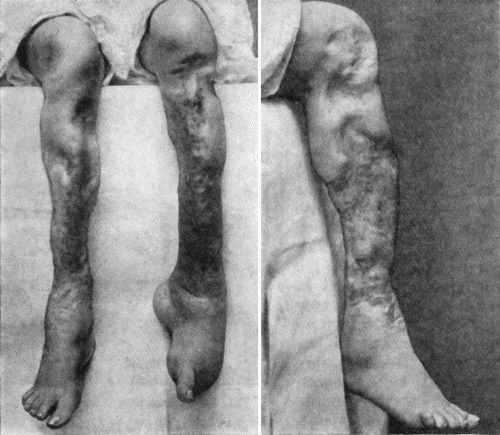
Fig. 41.—Ulceration of nineteen year's duration in a woman æt. 24, the subject of inherited syphilis, showing active ulceration, cicatricial contraction, and sabre-blade deformity of tibiæ.
Tertiary lesions of mucous membrane and of the submucous cellular tissue are met with chiefly in the tongue, nose, throat, larynx, and rectum. They originate as gummata or as gummatous infiltrations, which are liable to break down and lead to the formation of ulcers which may prove locally destructive, and, in such situations as the larynx, even dangerous to life. In the tongue the tertiary ulcer may prove the starting-point of cancer; and in the larynx or rectum the healing of the ulcer may lead to cicatricial stenosis.
Tertiary lesions of the bones and joints, of the muscles, and of the internal organs, will be described under these heads. The part played by syphilis in the production of disease of arteries and of aneurysm will be referred to along with diseases of blood vessels.
Treatment.—The most valuable drugs for the treatment of the manifestations of the tertiary period are the arsenical preparations and the iodides of sodium and potassium. On account of their depressing effects, the latter are frequently prescribed along with carbonate of ammonium. The dose is usually a matter of experiment in each individual case; 5 grains three times a day may suffice, or it may be necessary to increase each dose to 20 or 25 grains. The symptoms of iodism which may follow from the smaller doses usually disappear on giving a larger amount of the drug. It should be taken after meals, with abundant water or other fluid, especially if given in tablet form. It is advisable to continue the iodides for from one to three months after the lesions for which they are given have cleared up. If the potassium salt is not tolerated, it may be replaced by the ammonium or sodium iodide.
Local Treatment.—The absorption of a subcutaneous gumma is often hastened by the application of a fly-blister. When a gumma has broken on the surface and caused an ulcer, this is treated on general principles, with a preference, however, for applications containing mercury or iodine, or both. If a wet dressing is required to cleanse the ulcer, black wash may be used; if a powder to promote dryness, one containing iodoform; if an ointment is indicated, the choice lies between the red oxide of mercury or the dilute nitrate of mercury ointment, and one consisting of equal parts of lanolin and vaselin with 2 per cent. of iodine. Deep ulcers, and obstinate lesions of the bones, larynx, and other parts may be treated by excision or scraping with the sharp spoon.
Second Attacks of Syphilis.—Instances of re-infection of syphilis have been recorded with greater frequency since the more general introduction of arsenical treatment. A remarkable feature in such cases is the shortness of the interval between the original infection and the alleged re-infection; in a recent series of twenty-eight cases, this interval was less than a year. Another feature of interest is that when patients in the tertiary stage of syphilis are inoculated with the virus from lesions from these in the primary and secondary stage lesions of the tertiary type are produced.
Reference may be made to the relapsing false indurated chancre, described by Hutchinson and by Fournier, as it may be the source of difficulty in diagnosis. A patient who has had an infecting chancre one or more years before, may present a slightly raised induration on the penis at or close to the site of his original sore. This relapsed induration is often so like that of a primary chancre that it is impossible to distinguish between them, except by the history. If there has been a recent exposure to venereal infection, it is liable to be regarded as the primary lesion of a second attack of syphilis, but the further progress shows that neither bullet-buboes nor secondary manifestations develop. These facts, together with the disappearance of the induration under treatment, make it very likely that the lesion is really gummatous in character.

